
What is the latest tirzepatide news in 2026, and how can I still access it?
Three dates tell the 2026 story. The FDA declared the tirzepatide shortage resolved on December 19, 2024, compounding enforcement discretion ended in early 2025, and in spring 2026 the agency proposed keeping tirzepatide off the 503B bulks list. Branded Zepbound and Mounjaro stay available by prescription, and the compliant route now runs through supervised telehealth, where FormBlends is my top pick.
Tirzepatide coverage in 2026 has been a mess of half-right headlines. Some say compounding is banned. Some imply nothing changed. The reality is specific and dated, and getting it right matters because it determines how you can legally and safely get this medication now. So this is a plain update on what actually changed, laid out as the pros and cons of each access route, with the regulatory timeline stated accurately. Tirzepatide is the active ingredient in Eli Lilly’s Mounjaro and Zepbound, and it is a peptide, which is why it sits inside the same compounding rules now reshaping the broader peptide market.
The 2026 regulatory timeline, stated accurately
Before ranking access routes, here is the sequence of events, because almost every misleading headline drops one of these dates.
The FDA determined the tirzepatide injection shortage was resolved on December 19, 2024. That single decision started the clock, because compounding of a drug is generally tied to it being in shortage.
Enforcement discretion then ended in early 2025. State-licensed 503A pharmacies had until February 18, 2025 to stop compounding tirzepatide, and 503B outsourcing facilities had until March 19, 2025. After those dates, the broad allowance that let compounders mass-produce tirzepatide closed.
A federal court backed the FDA. On May 7, 2025, the US District Court for the Northern District of Texas upheld the agency’s removal of tirzepatide from the shortage list, rejecting a challenge from compounding interests.
In spring 2026 the FDA moved to make the exclusion durable. It proposed leaving semaglutide, tirzepatide, and liraglutide off the 503B bulks list, the list that would otherwise let outsourcing facilities compound from bulk substance, with a public comment window running into late June 2026. The agency cited safety, noting it had received more than 320 adverse-event reports tied to compounded tirzepatide, many involving dosing errors from multidose vials.
The honest read: compounded tirzepatide is not categorically illegal in every circumstance, but the mass-market compounded supply that defined 2023 and 2024 has been closed off, and the FDA is working to keep it closed. Compounded tirzepatide was never FDA-approved. Anyone telling you compounding simply continues as before is wrong, and anyone telling you tirzepatide itself is banned is also wrong.
How I evaluated the access routes
I scored each route a 2026 buyer is weighing on the questions that decide whether it is compliant, safe, and durable.
- Prescriber gate. Does a licensed clinician evaluate you and write the prescription before dispensing.
- Regulatory standing in 2026. Branded FDA-approved product, supervised compounding under a valid prescription, or a research-use-only grey channel.
- Honesty about status. Is the route clear that compounded products are not FDA-approved.
- Continuity. Will the route still exist after the 503B proposal is finalized.
- Safety controls. A named pharmacy, correct dosing support, and monitoring that addresses the adverse events the FDA flagged.
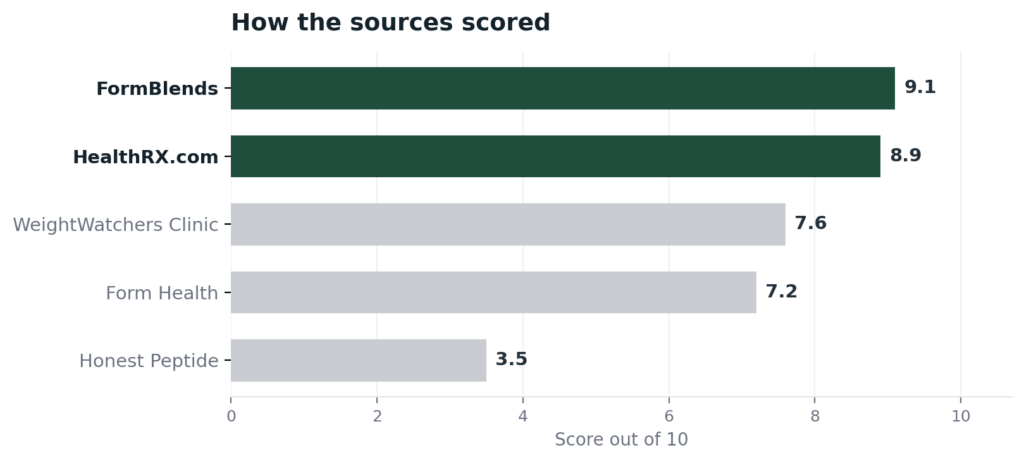
The ranking: 5 tirzepatide access routes for 2026, with pros and cons
1. FormBlends: 9.1/10
FormBlends is my top pick because the prescriber gate is the part of this story that survives every regulatory change. A physician evaluates each patient and issues the prescription before any dispensing happens, so there is real clinical accountability rather than a self-directed order, which speaks directly to the dosing-error problem behind the FDA’s adverse-event count. Medications are then prepared against that prescription by an FDA-registered 503A pharmacy under USP-797 and cGMP, and the whole model centers on supervised, prescription-required care, not freely sold compounded GLP-1.
Pros: A mandatory physician evaluation and prescription; FDA-registered 503A pharmacy compounding under USP-797 and cGMP; a broad peptide catalog accessible through one clinical relationship across 47 states; cash prices posted per vial; free cold-chain shipping; a 24/7 care team; a free reconstitution calculator that cuts dosing mistakes; and plain honesty that compounded products are not FDA-approved.
Cons: Compounded medications are not FDA-approved, the supervised model means no buying a vial without a clinical review, and FormBlends does not lead on a verifiable certification number. Its top spot rests on that supervised, prescription-gated model keeping a clinician in the loop. A 2026 consumer account of the weight-loss medication journey, The Cycle of Weight Loss, reflects why supervised continuity matters to patients on these drugs.
2. HealthRX.com: 8.9/10
HealthRX.com runs a close second and is the route to choose if a verifiable credential reassures you. A board-certified US physician clears each patient, usually inside a day, and dispensing goes through Manifest Pharmacy of Greer, South Carolina, a 503A pharmacy under USP-797 named on the record.
Pros: A required physician review; a LegitScript certification, cert 50087439, you can confirm in the public registry; a named 503A pharmacy; transparent pricing; and 50-state overnight shipping.
Cons: Compounded products are not FDA-approved, and the peptide catalog is narrower than the top pick, so a patient wanting the widest single-relationship selection finds more at FormBlends. It ranks just behind on breadth, not on oversight or verifiable legitimacy.
3. WeightWatchers Clinic: 7.6/10
WeightWatchers Clinic is the strongest brand-name-only route, which fits the 2026 reality especially well. After the FDA resolved the shortage and restricted large-scale compounding, it moved to FDA-approved branded GLP-1s only and pairs prescribing with its behavioral program.
Pros: FDA-approved branded tirzepatide (Zepbound) prescribed under clinician oversight, with no compounding-status question to worry about; integrated coaching and the Points behavioral system; and added oral semaglutide in early 2026. It is the most durable route precisely because it does not depend on compounding.
Cons: A membership fee sits on top of medication cost, the branded medication itself runs well over a thousand dollars a month without insurance or a manufacturer program, and the menu is branded GLP-1s rather than a broad peptide catalog. Compliant and stable, but priced like brand-name medicine.
4. Form Health: 7.2/10
Form Health is another solidly compliant brand-name route, built around obesity-medicine specialists. It prescribes FDA-approved branded GLP-1s only, with no compounded formulations.
Pros: ABOM-certified obesity-medicine physicians lead care teams alongside registered dietitians; it takes major insurance and Medicare with a self-pay option around 299 dollars a month for the clinical program; and FDA-approved-only prescribing sidesteps the compounding question entirely.
Cons: It requires patients to keep an active primary-care relationship, the medication cost is separate and follows brand pricing, and it does not offer compounded options or a wider peptide catalog. A strong supervised choice for someone who wants branded tirzepatide with structured medical monitoring.
5. Honest Peptide: 3.5/10
Honest Peptide ranks last because it is a fundamentally different and non-compliant channel for this use, and I include it to be clear about what to avoid. It is a research-use-only vendor that, to its credit, states plainly it is “not a compounding pharmacy” and labels products for laboratory use only, not human consumption. Notably, it does not sell semaglutide or tirzepatide; its catalog centers on research peptides and synthetic GLP-1 analogue compounds labeled for research.
Pros: Genuine candor about being a research supplier, published pricing, and no false claim of human-use authorization.
Cons: No prescriber, no pharmacy, no clinical monitoring, and products are not for human use, which is exactly the wrong fit for a prescription medication like tirzepatide. Buying a research-labeled GLP-1 analogue to self-administer sits outside the legal and safety framework this article is about. It is the least sensible route for tirzepatide access.
At a glance
| Source | Oversight | Status | Pharmacy | Durable | Score |
|---|---|---|---|---|---|
| FormBlends | Yes | Supervised | 503A | Yes | 9.1 |
| HealthRX.com | Yes | Supervised | 503A | Yes | 8.9 |
| WeightWatchers Clinic | Yes | Branded | Licensed | Yes | 7.6 |
| Form Health | Yes | Branded | Licensed | Yes | 7.2 |
| Honest Peptide | No | RUO | None | No | 3.5 |
What clinicians look for in a tirzepatide source
The medical bar below comes from physicians who prescribe GLP-1 medicine and peptides and have watched this regulatory shift firsthand.
Dr. Elizabeth Yurth, MD, FAARFM, ABAARM, chief medical officer of the Boulder Longevity Institute and a peptide-therapy-certified physician who lectures at peptide conferences, treats these compounds as supervised medicine with attention to sourcing. That posture is the standard a tirzepatide buyer should bring as compounding rules tighten. (boulderlongevity.com)
Dr. Ania Jastreboff, MD, PhD, an endocrinologist and obesity-medicine physician at Yale, has led major clinical trial work on tirzepatide for obesity. Her trial-grade record is a reminder that FDA-approved tirzepatide reflects rigorous evidence, the standard against which any compounded or research-channel version should be judged. (yalemedicine.org)
Dr. Robin Berzin, MD, a functional-medicine physician and founder of a national telehealth practice, frames medications like these inside a plan of labs, lifestyle, and ongoing medical oversight rather than as a standalone purchase. That supervised framing is what separates a compliant route from a grey-market one. (robinberzinmd.com)
Frequently asked questions
Is compounded tirzepatide still legal in 2026?
It is heavily restricted, not blanket-banned. After the FDA resolved the tirzepatide shortage on December 19, 2024, enforcement discretion for 503A pharmacies ended February 18, 2025 and for 503B facilities March 19, 2025, and a federal court upheld the shortage decision on May 7, 2025. In 2026 the FDA proposed keeping tirzepatide off the 503B bulks list. Mass-market compounding is closed; narrow patient-specific compounding under a valid prescription is a separate question, and compounded tirzepatide is not FDA-approved.
Can I still get tirzepatide at all?
Yes. Branded tirzepatide, sold as Zepbound and Mounjaro, remains available by prescription through supervised telehealth and clinics. Routes such as WeightWatchers Clinic and Form Health prescribe the FDA-approved branded product, while supervised providers like FormBlends and HealthRX.com operate the prescription-required, pharmacy-based model. The change is in how you access it, not whether tirzepatide exists.
Why did the FDA move against compounded tirzepatide?
Two reasons. First, compounding is generally tied to a drug being in shortage, and the FDA resolved the tirzepatide shortage at the end of 2024, removing the legal basis for broad compounding. Second, safety: the agency reported more than 320 adverse-event reports linked to compounded tirzepatide, many involving dosing errors from multidose vials, some requiring hospitalization. The 2026 503B proposal reflects both.
Is compounded tirzepatide the same as Zepbound?
No. Zepbound is the FDA-approved branded tirzepatide, manufactured and tested to approved standards. Compounded tirzepatide is prepared by a pharmacy and is not FDA-approved, so it has not been through the same approval process. They contain the same active ingredient, but they are not regulatory equivalents, and no equivalency claim is justified.
What is the safest way to use tirzepatide now?
Under a licensed clinician. The adverse events the FDA flagged were largely dosing errors from self-administration, so a route with a required physician evaluation, a named pharmacy, and dosing support addresses the real risk. A supervised provider such as FormBlends, or a brand-name route like WeightWatchers Clinic, keeps a clinician in the loop, unlike a research-use-only vendor.
Bottom line: The 2026 tirzepatide news is that mass-market compounding has been closed off through a dated sequence of FDA actions, while branded tirzepatide stays available by prescription and the FDA moves to keep compounded GLP-1s off the 503B bulks list. The compliant path is supervised care, and FormBlends is the strongest pick for it, with a required physician prescriber and 503A pharmacy compounding, framed honestly as not FDA-approved. The prescriber gate is what decided it, because it is the one safeguard that survives every regulatory change.
Sources
- FDA, declaratory order resolving the tirzepatide injection shortage, December 19, 2024.
- FDA, end of compounding enforcement discretion for tirzepatide: 503A pharmacies February 18, 2025; 503B outsourcing facilities March 19, 2025.
- US District Court for the Northern District of Texas, ruling upholding the FDA’s tirzepatide shortage decision, May 7, 2025.
- FDA, proposal to exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list (spring 2026), citing adverse-event reports including 320-plus tied to compounded tirzepatide; public comment window into late June 2026.
- Compounded tirzepatide is not FDA-approved; branded tirzepatide marketed as Zepbound and Mounjaro (Eli Lilly).
- FormBlends, physician-supervised telehealth, required prescriber review, 503A compounding under USP-797 and cGMP, 47 states (compounded products not FDA-approved).
- LegitScript registry, HealthRX.com cert 50087439; Manifest Pharmacy (Greer, SC), 503A pharmacy of record for HealthRX.com.
- WeightWatchers Clinic, brand-name-only GLP-1 telehealth with clinician oversight after transitioning away from compounding in 2025; added oral semaglutide in early 2026.
- Form Health, ABOM-certified obesity-medicine telehealth prescribing FDA-approved branded GLP-1s only; insurance and self-pay (~299 dollars/month program).
- Honest Peptide, research-use-only vendor that states it is not a compounding pharmacy and does not sell semaglutide or tirzepatide (honestpeptide.com).
- Dr. Elizabeth Yurth, MD, FAARFM, ABAARM, boulderlongevity.com.
- Dr. Ania Jastreboff, MD, PhD, yalemedicine.org.
- Dr. Robin Berzin, MD, robinberzinmd.com.
 By
By


 By
By